


Navigating the Vaccine Question
None of this is meant as medical advice. Think for yourself.

Vaccines are a uniquely touchy subject. Government agencies and many doctors consider them an essential keystone of public health. Without vaccines, the argument goes, we would still be faced with thousands of deaths and injuries from measles, whooping cough, and polio. Conversely, some parents and doctors see them as unnecessary interventions laden with toxic ingredients, potentially sparking the surge of chronic diseases and allergies that have skyrocketed in recent decades, such as autism, ADHD, allergies, and asthma.
Who's right? As parents, we want to do what's best for our children. We are responsible for their health. If they’re sick, we take care of them until they get better. We go to great lengths to make sure they have healthy, natural food, free from pesticides and questionable additives.
I think that understanding the issues behind vaccines---whether or not to get them, and which, if any, to get---is just as important. We can't make a good decision unless we have all of the relevant information. So I've tried to compile the information from the best sources and summarize what they say.
Are Vaccines Safe and Effective?
One mainstay of vaccine conversation is that vaccines are "safe and effective." Safe, meaning they have a low or tolerable risk of death, hospitalization, or injury; or at least a well-understood set of risks. Effective, meaning they inoculate recipients from the risk of receiving the targeted disease.
No Safety Trials
The "gold standard" of pharmaceutical trials is a double-blinded randomized, controlled trial using an inert placebo. Unfortunately, no vaccine on the childhood schedule has completed such a trial. Typically, vaccines are tested against older vaccines. Those vaccines in turn were tested against even older vaccines, or they were never subjected to a controlled trial at all. Sometimes, a vaccine is "tested" against the same formulation minus a single antigen.
Obviously, this kind of test cannot discern whether the vaccine is safe, only perhaps if it’s as safe as older vaccines. Specifically, it doesn't clarify whether a vaccine's adjuvants -- toxic substances which are intended to stimulate an immune response -- cause side effects like paralysis, allergies, seizures, fevers, or neurological diseases.

The trials that do occur are limited by their relatively small size and short duration. Given the fact that controlled trials are not conducted, the definitive scientific evidence to say “do not cause” specific diseases largely does not exist.
Nevertheless, the CDC glibly declares “Vaccines do not cause autism,” and cites a report written by the Institute of Medicine:

Source: CDC. Autism and Vaccines. https://www.cdc.gov/vaccinesafety/concerns/autism.html
I decided to read the report for myself to verify their claim. The authors of the report evaluated the safety of 8 vaccines. They were asked to read all of the available medical literature and determine whether or not there was evidence tying vaccines to certain conditions, like autism. They largely found the required evidence to make a determination didn’t exist. For 7 out of 8 vaccines the authors did not address or found the evidence was inconclusive regarding whether they cause autism. Summarizing that evidence as “vaccines do not cause autism” is unscientific and unsupported by the report the CDC itself cited.
From the report:

Source: IOM. Adverse Effects of Vaccines. 2012. FR: Favors Rejection. Blank: Did not address. I: Inconclusive.
The report authors further clarify in the case of the DTaP vaccine:
The epidemiologic evidence is insufficient or absent to assess an association between [the DTaP] vaccine and autism.
I found it remarkable that the CDC would cite this report to prove vaccines don’t cause autism when it says in fact that we can’t know with the available evidence.
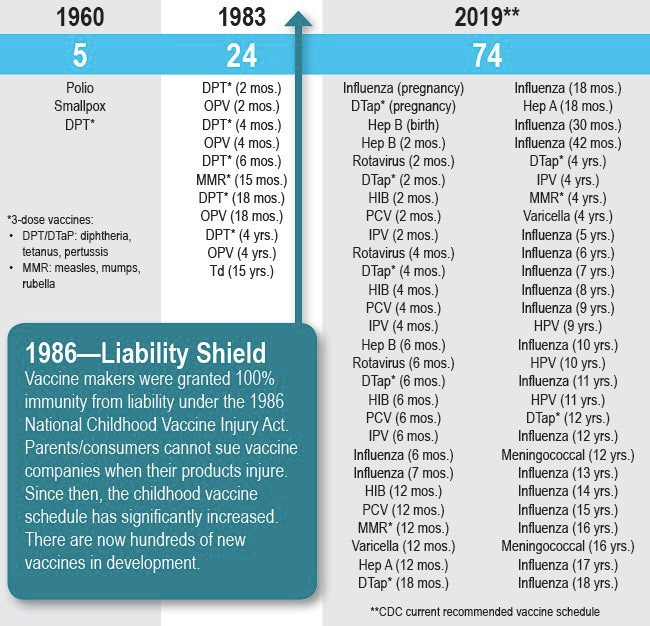
Liability Shield
In 1986, the U.S. Government indemnified vaccine manufacturers against any damage their products would cause. So, no matter how much harm a vaccine may cause, the manufacturer can never be held liable. The government was induced to take this extraordinary step after pharmaceutical companies claimed vaccines were "unavoidably unsafe" and threatened to stop manufacturing them. Even though vaccine mandates guaranteed a large market, the cost of compensating victims who were injured by vaccines made selling them insufficiently profitable by the manufacturers’ standards.
In exchange for this blanket liability protection, the Department of Health and Human Services promised to conduct safety reviews every two years and report them to Congress. Unfortunately, it appears they haven’t followed through on that obligation. After being sued to produce these records, in 2018 HHS admitted they had never conducted any of the required safety testing and never issued a report to Congress as required by law.
The lack of adequate safety testing combined with a large, guaranteed market without any risk of having to compensate patients for injuries has led to a booming vaccine market and a rapidly growing vaccine schedule. Unfortunately, it may have also led to a large number of vaccine injuries.
Evidence of Vaccine Danger
Every licensed vaccine is required to include an insert disclosing side effects seen in trials. While manufacturers can claim that these side effects are equally prevalent in the “control” group (which, as reviewed earlier, is vaccinated as well), they still must disclose them.
If, later, vaccine recipients experience a subset of these adverse effects shortly after being vaccinated, they may petition a special vaccine injury court for compensation. Most parents aren’t aware of this program, and the standards for having a case be seen and eventually compensated are highly restrictive. For example, there are only three injuries eligible for compensation from the Hepatitis B vaccine, and they must be observed and documented to have occurred by a medical professional within 1, 4 or 48 hours of vaccination respectively to be eligible for compensation. Additionally, the parents must find a lawyer who is willing to represent them in a lengthy dispute and file a case within a limited time window to be seen by the court.
Even with all of these restrictions, the program has paid out over $4.5B, with hundreds of millions of dollars going to vaccine injury victims every year. There have been 26,138 cases filed for death and injury from vaccines, and 9,825 have received compensation.
In that same time period, perhaps around 100M people have gone through the childhood vaccination schedule. If vaccine injuries were “1 in a million” as is occasionally claimed by vaccine advocates, we would see about 100 people injured, and a small fraction of those would likely be compensated.

In 1998, several doctors reviewed a subset of this data. They looked into cases of children who were brain damaged or died shortly after receiving the MMR vaccine. After looking at the files of 48 children, eight of whom died and the remainder of whom had lifelong mental disabilities like retardation, chronic seizures, or paralysis, they found that the children’s cases were strikingly similar. Most experienced symptom onset on the same few days, and all of the cases involved the measles vaccine. They concluded that the measles vaccine was likely responsible for these childrens’ brain damage and death.
Reports of vaccine injuries and deaths are also made in the VAERS system, which is a passive surveillance system run jointly by the FDA and the CDC. Most reports are made by nurses, doctors, and other medical professionals, and submitting a fraudulent report is illegal and punishable as a felony. Since the system is not widely known and reports are time-consuming to make, this too captures only a portion of vaccine injuries. An automatic surveillance system when tested on an identical patient population estimated 10-100x more vaccine associated injuries occurred than were reported into VAERS. Nevertheless, tens of thousands of vaccine injuries are reported every year.

Pirate Trials
While government agencies (who would bear massive liabilities if vaccines were shown to cause harm) have not funded any trials comparing vaccinated to unvaccinated populations, there have been several conducted by independent groups. In all cases, they generate a firestorm of controversy by demonstrating injuries like autism, allergies, and other chronic diseases occur at much higher rates in vaccinated populations compared to unvaccinated populations. And, without exception, they face fierce criticism and backlash from official authorities, even resulting in their authors’ medical licenses getting revoked or the journals retracting papers.
Before getting into the controversy, let’s take a look at the results:

Lyons-Weiler J, Thomas P. Relative Incidence of Office Visits and Cumulative Rates of Billed Diagnoses Along the Axis of Vaccination. Int J Environ Res Public Health. 2020 Nov 22;17(22):8674. doi: 10.3390/ijerph17228674. Retraction in: Int J Environ Res Public Health. 2021 Jul 22;18(15): Erratum in: Int J Environ Res Public Health. 2021 Jan 22;18(3): PMID: 33266457; PMCID: PMC7709050.

Hooker BS, Miller NZ. Analysis of health outcomes in vaccinated and unvaccinated children: Developmental delays, asthma, ear infections and gastrointestinal disorders. SAGE Open Medicine. 2020;8. doi:10.1177/2050312120925344
Summarizing their results, these studies found a significant association between vaccines and neurological issues like ADHD and autism. They found the vaccinated were 2-4 times more likely to have these neurodevelopmental disorders than their unvaccinated peers. They also found the vaccinated were much more likely to have “autoimmune” conditions like asthma and allergic sensitivities. According to all of the studies, the vaccinated were more susceptible to chronic infections.
These studies attracted quite a bit of controversy. The “Pilot” study was retracted, and then accepted to another journal. The initial journal didn’t give a reason for the retraction, and instead denied they had accepted the publication in the first place. None of the data were called into question.
The “Office Visit” study was retracted because, to quote the editors, “concerns were brought to the attention of the editorial office regarding the validity of the conclusions of the published research…Adhering to our complaints procedure, an investigation was conducted that…confirmed that the conclusions were not supported by strong scientific data.” While this statement may sound reasonable on its face, a moment of reflection reveals it to rely upon a strange and tortured logic. The journal didn’t find any issues with the validity or accuracy of the data in the study, but because the editorial staff found the implications of those data inconsistent with the scientific consensus, they decided it must be retracted. Following this example as a general practice would halt all scientific progress and freeze the current consensus into an unalterable paradigm.
There have been other studies which have compared vaccinated versus unvaccinated children and the incidence of chronic diseases. Here is a list of seven such studies I was able to find. I summarized the findings across them for a few select diseases in a chart.

The results are clear and have a high degree of corroboration across studies. Vaccinated children are much sicker than unvaccinated children. They have a higher incidence of chronic diseases like allergies, ADHD, asthma, autism, and frequent infections. Each of these findings has been replicated in at least three independent studies. Certain studies also found vaccinated children were more commonly inflicted with Eczema, Learning Disabilities, Neurodevelopmental Disorders, Pneumonia, Ear Infections, GI Disorders, Asthma, Developmental Delays, Fevers, Pink Eye, Breathing Issues, Eating Disorders, Respiratory Infections, Behavioral Issues, Anemia, Throat inflammation, Convulsions, Infections, Seizure, Hospitalization, Sleep Issues, and Speech Disorders (see collected data here).
Finally, a recent survey of 10,000 parents showed an association of vaccine shots with ADHD and autism diagnosis. The more shots given, the likelier a diagnosis of a developmental disorder.
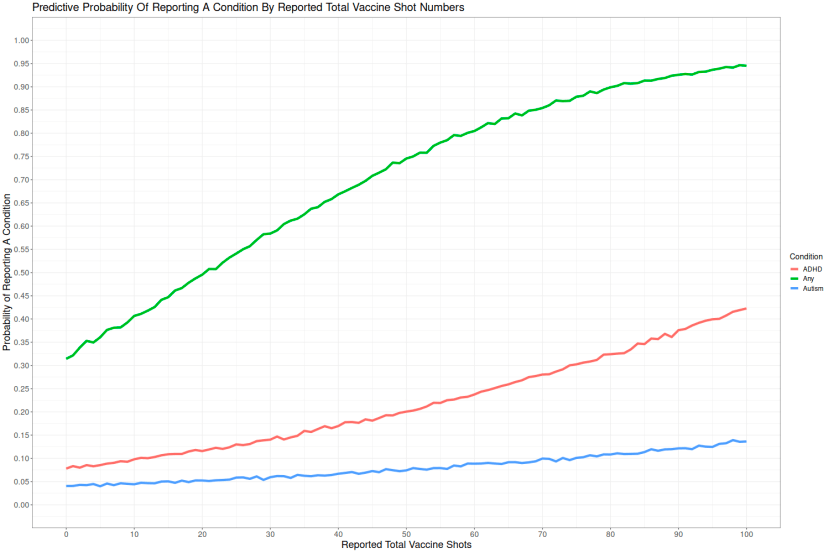
This evidence is particularly compelling because the risk appears to be additive and monotonically increasing as more shots are given.
In summary, while we do not have the highest quality randomized controlled trials conclusively showing vaccines cause autism, ADHD, and other chronic diseases, there is a large and cohesive body of research that implicates them.
Theories of Injury
How could vaccines hurt children? The most obvious explanation is that they contain toxic ingredients. These ingredients are called “adjuvants” and are intended to stimulate the immune system. The immune system is most stimulated when it senses a foreign or toxic substance, so adjuvants generally consist of a soup of toxic substances. Here are some ingredients used in vaccines:
Aluminum (implicated in brain damage and neurodegenerative diseases)
Formaldehyde (carcinogenic, banned in Europe)
Beta-Propiolactone (carcinogenic)
GMO Yeast, Bacterial and Viral DNA, Dairy/Egg Components (can cause allergies)
Glutaraldehyde (can cause birth defects in animals)
Peanut & Soybean Oil (can create allergies)
Animal and Human Cells (foreign substances can cause rejection, leukemia, diabetes)
Mercury (highly toxic)
MSG (linked to birth defects, developmental delays, infertility, banned in Europe)
Neomycin Sulphate (interferes with B6 absorption)
Phenol/Phenoxyethanol (antifreeze, toxic)
Polysorbate 80 & 20 (carcinogenic)
Tri(n) Butylphosphate (possibly renotoxic)
Here is a list of excipients for each vaccine:

There is substantial evidence that in addition to provoking an immune response, some of these excipients may be causing unintended side effects.
Allergies
When scientists want to give an animal a peanut allergy in the lab, they stimulate the animal’s immune system with a toxin while feeding them peanuts. The animal’s immune system associates the toxin with the peanuts, and so becomes sensitized to peanuts. It is not unreasonable to suggest the same thing happens in humans. Perhaps this explains the rising incidence of peanut allergies after they’ve been injected alongside adjuvants in vaccines.

Todd A. Mahr, Jay A. Lieberman, Tmirah Haselkorn, Varsha Damle, Yasser Ali, Arul Chidambaram, Noelle M. Griffin, J. Wesley Sublett, Characteristics of Peanut Allergy Diagnosis in a US Health Care Claims Database (2011-2017), The Journal of Allergy and Clinical Immunology: In Practice, Volume 9, Issue 4, 2021, Pages 1683-1694.e5, ISSN 2213-2198, https://doi.org/10.1016/j.jaip.2020.12.020.
Aluminum Toxicity
When questioned about the quantity of aluminum adjuvants in vaccines and their potential toxicity, the prominent vaccine advocate Dr. Paul Offit stated, “Parents can be reassured that the trace quantities of aluminum in vaccines can’t possibly do harm.” He clarifies this is because the amount of aluminum in vaccines is incredibly small:
“…you are much more likely to have aluminum in your circulation if you inject it than if you ingest it. But the point is that there’s so much more aluminum in the environment, either in the food you eat or the water you drink, than you would ever get as a shot in vaccines..”
Unfortunately, this claim is far from accurate. As Offit himself states, aluminum is much more efficiently absorbed when it is injected into the body versus when it is eaten. When ingested, the body efficiently filters out aluminum in the GI tract and prevents its absorption, allowing only 0.1%-0.3% into the body.
Vaccines given in the first six months of life per the CDC childhood schedule contain 3,675 mcg of aluminum. Aluminum found in an infant’s breast milk may be as much as 7 mg in the first 6 months of life, up to 21 mcg of which will be absorbed. That means there’s 175 times more aluminum exposure from vaccines compared to breast milk.
Aluminum serves no function in the body. It is neurotoxic, neurodegenerative, toxic to bone tissue, and may contribute to autoimmune disorders. In the 1990s, there were reports of babies dying and becoming developmentally impaired after receiving IVs contaminated with aluminum, which led to the FDA setting a limit on daily aluminum exposure. According to the FDA, they should be limited to 4-5 mcg/kg/day, and even these levels can cause toxicity. That is equivalent to a limit of 20 mcg for an 8lb baby or 50 mcg for a 20lb baby. There is no aluminum-containing vaccine on the schedule which is below this limit.

The evidence for aluminum’s toxicity is vast. The article “Aluminum in Childhood Vaccines Is Unsafe” in the Journal of American Physicians and Surgeons provides a survey of the havoc aluminum wreaks upon the body:
Aluminum is neurotoxic and has a long history of well documented hazards. For example, as early as 1921 The Lancet described a 46-year-old metal worker in whom “[aluminum] produced a rather slow intoxication. In this case it caused memory loss, tremor, jerky movements and incontinence of urine.
According to the American Academy of Pediatrics (AAP), “Aluminum is now being implicated as interfering with a variety of cellular and metabolic processes in the nervous system and in other tissues.
aluminum is a widely recognized neurotoxin that inhibits more than 200 biologically important functions and causes various adverse effects in plants, animals, and humans.
A recent paper by Tomljenovic and Shaw affirmed that aluminum is a neurotoxin and may be a co-factor in several neurodegenerative disorders and diseases, including Alzheimer’s, Parkinson’s, multiple sclerosis, amyotrophic lateral sclerosis (ALS), autism, and epilepsy
Recent data by Perricone et al. showed that aluminum adjuvants in vaccines have been linked to multiple sclerosis, systemic lupus erythematosus, chronic fatigue syndrome, Gulf War syndrome, macrophagic myofasciitis, arthritis, and autoimmune/inflammatory syndrome induced by adjuvants (ASIA syndrome), an autoimmune disease with neurological and cognitive manifestations
Some people develop macrophagic myofasciitis (MMF) after receiving an aluminum-containing vaccine. MMF is characterized by an aluminum-filled lesion (wound) at the site of an earlier vaccination…it is a systemic ailment. Symptoms include chronic fatigue, chronic diffuse myalgia (muscle weakness), arthralgia (joint pain), and disabling headaches. Aluminum’s toxic effects can also manifest as impaired psychomotor control, repetitive behavior, speech disorders, sleep disturbances, seizures, confusion, and anxiety, as well as deficits of concentration, learning, and memory. Nearly 20% of patients with MMF develop an autoimmune disease, including neuromuscular and multiple sclerosis-like demyelinating disorders
German researchers documented MMF in a 3-month old East Indian child following his hepatitis B vaccine at birth, “after which he developed generalized hypotonia, and central nervous system and peripheral nervous system manifestations at one month of age. The child also had respiratory failure, decreased spontaneous movements, apnea spells, and generalized seizures.”
According to Canadian MMF researchers, “aluminum has been demonstrated to impact the central nervous system at every level, including by changing gene expression…based on the current and emerging literature, it seems unlikely that in the future aluminum will be considered safe for human use in any of the current medicinal applications.”
The Journal of Inorganic Biochemistry published data showing a highly significant positive linear correlation between the amount of aluminum infants receive from their vaccines and the rates of autism…“Our results...suggest that a causal relationship may exist between the amount of aluminum administered to preschool children at various ages through vaccination and the rising prevalence of autism spectrum disorders.”
Given the widespread and highly suggestive evidence of aluminum’s toxicity, and the difficulty babies have in safely excreting it once injected, it seems unconscionable to intentionally expose a baby to this toxin without clear and convincing evidence of a much greater benefit.
Vaccine Benefits
At best, vaccines provide “sterilizing immunity” to their target diseases. That means they are 100% effective at preventing the vaccinated from contracting the disease. The benefit, in that case, is avoiding the risk of hospitalization, death, or permanent disability that comes with being infected with the disease multiplied by the risk of being infected in the first place. It can be conceptualized with the following equation:
Net Benefit of Vaccine = (Risk of Contracting Disease) x (Risk of Death/Hosp./Disability from Disease) x (Effectiveness of Vaccine) - (Risk of Death/Hosp./Disability from Vaccine)
For each of the vaccines in the schedule, I will make an effort to estimate each of these factors.
Hepatitis B
Risk of contracting Hepatitis B is very low, and generally restricted to those who engage in IV drug use and highly promiscuous sexual activity. If contracted, the danger from hepatitis B is low, with over 99% having a full recovery and lifelong immunity.
From the National Vaccine Information Center:
Fifty percent of adults infected with hepatitis B will have no symptoms. Hospitalization for acute hepatitis B is low and limited to the elderly, individuals with pre-existing medical conditions and those who require treatment for dehydration from severe nausea and vomiting. On very rare occasions, acute hepatitis B infections can lead to liver failure and death.
Approximately five percent of adults do not recover completely and will become chronic carriers of the virus. Of this number, only 15 percent will develop life-threatening liver disease such as cirrhosis or liver cancer.
Immunity from the hepatitis B vaccine wanes significantly. From Dr. Paul Thomas:
A 2013 study showed that by age sixteen, the majority of children—over 50 percent—who were given the hepatitis B vaccine as infants are no longer protected. A 2014 study published in Pediatrics found similarly poor immunity rates among sixteen-to-nineteen-year-olds vaccinated as infants. Only 24 percent of American teens who completed the three-shot series by age one had adequate protection. Giving the hepatitis B series of shots to newborns not only exposes them to toxic doses of aluminum, but also fails to give them lasting protection against hepatitis B.
The hepatitis B vaccine contains 225 mcg of aluminum, 5-10x the safe limit prescribed by the FDA. There have been 137,676 adverse events associated with the Hepatitis B vaccine reported to VAERS, including 2,337 deaths.
The balance of evidence seems to recommend against the hepatitis B vaccine.
Rotavirus
Rotavirus is usually a mild illness, the main risk of which is diarrhea leading to dehydration. This can be treated with IV fluids. If babies are nursing when they contract RV, their maternal antibodies generally protect them. Most babies have such mild symptoms that they are undetectable, and then gain immunity to the disease.
Since the vaccine has been introduced, new strains of rotavirus have emerged and possibly become dominant which are not fully protected against by the vaccine. The Cochrane Collaboration released a review of the vaccine’s effectiveness in 2019:
In low mortality countries, ROTARIX vaccine was reported to decrease the number of severe rotavirus infection by 84 percent and severe all-cause diarrhea infection by 41 percent. In the second-year post-vaccination, ROTARIX was found to decrease the rate of severe rotavirus infection by 82 percent and severe all-cause diarrhea infection by 37 percent. After three years, ROTARIX did not reduce the rates of severe rotavirus infection but one study found a 27 percent decrease in all-cause diarrhea infection. ROTARIX had no impact on reducing all-cause mortality rates in low mortality countries.
In low mortality countries in the first-year post vaccination, RotaTeq was found to decrease the rate of severe rotavirus infection by 92 percent but no data was collected to determine the vaccine’s impact on all-cause diarrhea rates. In the second year, RotaTeq was found to decrease the rate of severe rotavirus infection by 82 percent but again, no studies looked at the vaccine’s impact on all-cause diarrhea rates. RotaTeq had no impact on reducing all-cause mortality rates in low mortality countries.
The vaccine is a live virus, and so the side effects for the vaccine often mimic the disease itself. According to Dr. Paul Thomas: “Data from my own practice shows that those infants who got the rotavirus vaccine were four times more likely to have gastroenteritis and diarrheal illness than those who did not get the vaccine.”
There have been 53,091 adverse events associated with the rotavirus vaccine reported to VAERS, including 940 deaths.
Since the vaccine is waning in effectiveness, has no demonstrated effect on all-cause mortality, can cause the same symptoms as the disease itself, and the virus is easily treated if contracted and has a low mortality risk, the balance of evidence seems to recommend against the rotavirus vaccine.
Polio
The vast majority of polio cases, 95%, are asymptomatic. Less than 1% of polio cases result in paralysis, and about 2-5% of paralytic polio cases are fatal in children. The last case of polio contracted in the US occurred in 1979.
The poliovirus vaccine contains formaldehyde, a highly toxic and carcinogenic preservative. There have been 158,760 adverse events associated with the polio vaccine reported to VAERS, including 2,987 deaths.
Because the risk of contracting polio is so low, and it seems to have been largely eradicated through improved nutrition and health standards, and the vaccine contains questionable excipients, the balance of evidence seems to recommend against it.
Tetanus, Diphtheria, Pertussis/Whooping Cough
Tetanus and diphtheria are largely eradicated in the United States. From Dr. Paul Thomas:
There have been no deaths from diphtheria in children for at least thirty-five years. Your chance of getting diphtheria is less than 1 in 100 million.
The incidents of tetanus in children under five in over twenty-five years: 0.
Pertussis has a very high rate of recovery. According to the CDC:
During 2017, out of the 15,808 reported cases of pertussis there were 13 deaths, with 4 deaths occurring in children less than one year of age.
That means each year over 99.99% of people do not get diagnosed with pertussis, and of those who do get diagnosed more than 99.9% recover. Pertussis is most deadly to children under 3 months old.
The effectiveness of the DTaP vaccine is waning. From Dr. Paul Thomas:
Recent data suggests that the current acellular vaccines are not as effective in providing protection against whooping cough as they were even just a few years ago. Australia, with a population of nearly 24 million, had more than 150,000 cases of pertussis from 2008 to 2012, despite very high vaccine uptake rates for infants and children.
In one 2015 study of fully vaccinated teenagers in Washington State, researchers found that the Tdap vaccine was only 73 percent effective a year after vaccination and just 34 percent effective two to four years later, leading them to conclude that the “lack of long-term effectiveness may contribute to increases in pertussis among adolescents.”
Another study, published in 2016, found that during a whooping cough outbreak in a Florida preschool from September 2013 to January 2014, nearly 50 percent of the children who got sick with whooping cough were fully vaccinated.
The DTaP vaccine contains 170 mcg of aluminum. It also has pertussis toxin, which is one of the most lethal toxins in nature. It is intended to be in an “inactivated” form that can still “revert to toxicity” and cause brain inflammation, as well as the other symptoms of pertussis. There have been 181,269 adverse events associated with the DTaP vaccine reported to VAERS, including 3,302 deaths.
Because the vaccine is relatively ineffective, the target diseases are rare, and the vaccine may have serious side effects along with toxic ingredients, the balance of evidence seems to recommend against it.
Hib
Haemophilus Influenza Type B, or Hib, affects a small number of children, but has a substantial rate of injury and death. From the NVIC:
Prior to the introduction of vaccines targeting H. influenzae type b (Hib), between 0.5 and 3 percent of infants and children were found to have Hib present in the upper respiratory tract and Hib bacteria were rarely found in adults. Most children colonized Hib and developed immunity to it by the age of 6 as a result of being asymptomatic carriers. Currently, Hib is believed to colonize in the back of the throat of between 3 and 5 percent of children.
Prior to the introduction of Hib vaccines, children under the age of one accounted for approximately 60 percent of invasive Hib disease infections, with the majority of cases impacting infants between 6 and 11 months of age. Additionally, Hib meningitis was reported to be the most common presentation of invasive Hib disease and responsible for 50-65 percent of cases. An estimated 8,000 to 11,000 Hib meningitis cases occurred each year and 3 to 7 percent resulted in death. 15 to 30 percent of survivors had long-term neurological or hearing impairments as a result of the disease.
Hib vaccines seem to have short-term efficacy. Long term efficacy remains unknown. From Dr. Paul Thomas:
Postvaccine follow-up studies have shown a 71 percent decrease in Hib disease in under-five-year-olds from 1989 to 1991, and an 82 percent decrease in Hib meningitis between 1985 and 1991.
Hib vaccines have many reported side effects. According to the package insert, the adverse events were reported in patients given ActHib:
Tenderness, erythema, swelling, induration, fever, irritability, drowsiness, anorexia, unusual or persistent crying, vomiting, and seizure with apnea. Reported side effects post marketing have included convulsions, anaphylaxis, peripheral edema, extensive limb swelling, pruritus, and rash.
There have been 131,723 adverse events associated with the Hib vaccine reported to VAERS, including 2,885 deaths. These have one of the highest rates of VAERS reports per doses given.
Because there are substantial risks from both the disease and the vaccine, it’s hard to come to a decision on whether or not to recommend this vaccine. The balance of evidence doesn’t appear to strongly oppose or support its use.
Measles, Mumps, Rubella
Measles used to be so common it was thought of the same way our generation treated chicken pox. They had measles parties. It has an extremely low mortality rate, less than 1 in 10,000. And it generally affects badly only children with severe vitamin A deficiencies, and can be treated with doses of vitamin a. There have been no deaths from measles for over a decade.
Mumps is exceedingly rare as well. From Dr. Paul Thomas:
Though once a common childhood illness, we see very few cases of mumps in America nowadays. In 2014 there were 1,223 reported cases, and the year before only 584. Mumps is almost always a mild childhood illness. It can cause deafness (about 1 in 20,000) and brain swelling (1 in 6,000). Death from mumps is “exceedingly rare,” according to the CDC, and is much more likely to occur in adults than in children.”
Rubella is also a mild and rare illness. From Dr. Paul Thomas:
The rash that it causes looks like a mild form of measles and usually disappears within three to five days. Though up to 50 percent of rubella illnesses are so mild you do not even know you have one, symptoms usually include a mild fever, runny nose, and swollen glands before the telltale rash appears. Rubella is mildly contagious, spread from person to person through coughing and other secretions.
The last major outbreak of rubella occurred fifty years ago, in 1964–65. Today reported cases of rubella are exceedingly rare. In 2004 an independent panel of public health officials and infectious disease experts concluded that rubella had been eliminated from the United States, as another independent panel reiterated in 2011.
The MMR vaccine is one of the most associated with autism. From Dr. Paul Thomas:
I have more than a hundred families with children with severe autism, all of whom came to me after their children were diagnosed. Ask these parents about the MMR vaccine, and more than half will tell you they lost their child shortly after that vaccine.
There have been 141,073 adverse events associated with the MMR vaccine reported to VAERS, including 547 deaths.
Because there are substantial risks from the MMR vaccine, particularly the strong association with autism, and the potential diseases are rare, the balance of evidence appears to advocate against it.
Chicken Pox/Varicella
It’s chicken pox. It’s not a big deal.
Hepatitis A
It’s a very mild disease that rarely causes long-term damage. Most children, if infected, don’t show symptoms.
Unvaccinated Populations
Amish populations have a substantially lower rate of autism than the national average. They also vaccinate at a much lower rate than the public at large.
According to the CDC, 1 in 68 children, or 1.4% of children have autism as of 2014.
In 2010, researchers went door-to-door to assess the rate of autism among two Amish communities, screening 1899 children. They found The rate of autism at 1 in 271, a rate of 0.3%, which is ¼ the national average.
Dr. Max Wiznitzer, the neurologist of the largest Amish community in Ohio, reported the rate of autism in that community is 1 in 10,000, which is 140 times smaller than the national average.
Dr. Heng Wang, who is the medical director of the DDC Clinic in Middlefield, Ohio, suggested the rate is 1 in 15,000, which is 210 times smaller than the national average.
Moreover, the cases of autism that are found within Amish communities are either from children who received vaccinations or who have a clear genetic disorder. As far as I’m aware, there are no cases of “idiopathic” or “regressive” autism which has been growing rapidly in non-Amish communities.
Thank you so much for this article
Amazing research here. Everyone should know about this.